Women’s Health Has Worsened Since 1990
Según el artículo de Mattias Waller Lidström publicado en PLOS el 20/11/2017
Introduction
Self-rated health (SRH) is a widespread method of assessing health in populations and is an independent predictor of future morbidity, such as myocardial infarction, risk of diabetes, depression, rheumatic disease and sick leave; medical care utilisation; and mortality [1 2 3]. Two principal variants of SRH questions are often used: the general “How would you rate your health at present time?” and the comparative “How would you rate your health in comparison to others of the same age?” [4]. These are answered on a five- or three-level categorical scale. General and comparative SRH have similar associations with outcomes in cohort studies and with determinants in cross-sectional studies, but reflect different aspects of health and are not equivalent [4 5]. The comparative question contains in itself a reference for evaluations (compared to others) and steers the comparison to real persons and might thus be considered semantically clearer [6].
Gender issues are important in public health research. Gender is defined by the World Health Organization: “Sex refers to the biological and physiological characteristics that define men and women. Gender refers to the socially constructed roles, behaviours, activities, and attributes that a given society considers appropriate for men and women” [7]. Sweden is regarded as a country with a high level of gender equality in international comparison, and gender equality is an undisputable societal norm [8]. Still gender continues to play a considerable part in how work, wealth, power, and time use are distributed in the Swedish society [9]. Women in Sweden are gainfully employed to the same degree as men [9]. The Swedish labour market is however, gender-segregated; a large number of women work in the public sector, in caring and service professions, while men dominate in the private sector and work in areas such as construction and transportation [9]. Women earn less than men, despite being higher educated [9]. Women spend almost twice as much time as men performing household chores, and to a large extent shoulder the main responsibility for their families, including invisible tasks such as planning for everyday life to run smoothly, in addition to the caring of children and ailing or sick relatives [910]. Furthermore, women continue to be exposed to sexual, physical and psychological violence from their partners and former partners to a much higher degree than men [11].
International comparisons on self-reported items of health in several countries have been made based on WHO world health survey data [12 13]. Gendered differences in health could be seen in pooled data from all countries with women reporting worse health than men. Social determinants, mainly employment and education accounted for much of the differences although some of the differences were unexplained and presumably due to factors not in the model.
The situation in Sweden shows the same overall picture, women rating worse health than men, women having higher rates of sick listing particularly long term sick listing [14 15]. Johansson et al. investigated time trends of SRH from 1980 to 2005 in Sweden and found that SRH became poorer or was unchanged in those aged 16–47 but got better among person aged 48 or older [16]. Time trend for the period 1997–2006 indicated a highly prevalent, mental ill-health among the young in Stockholm County, a region representative of urbanized Western societies [17]. Swedish women in general and young women in particular report higher rates of anxiety and depression than men, both associated with poor SRH [9 14]. Concern has been raised over the increasing levels of anxiety and depressive emotions among young adults [17 18]. As we previously had done some work on comparative self-rated health and had access to a database from the Northern Sweden Monica study with time trends among young adults for comparative SRH and factors known to be associated with SRH we set out to investigate the issue. To the best of our knowledge, there are no studies using comparative self-rated health as an outcome variable among young adults in the Swedish setting. Several factors are associated with SRH. Among these we chose to investigate time trends of physical activity in leisure time; educational level; Body Mass Index (BMI); depressive feelings; anxiety; and satisfaction with economy. The rationale for this lies in the age group investigated where diseases on a population level play a minor role but habits reflected in BMI, physical activity, psychosocial factors, educational level, satisfaction with economy, feelings of depression and anxiety are factors that presumably play a greater role in SRH. These determinants have also been described in the Northern Sweden Monica study on a population basis for the ages 25–74 [14].
The aim of this article was to investigate time trends of comparative SRH over the period 1990 to 2014 in men and women aged 25–34 years. A secondary aim was to describe time trends of some determinants.
Research questions
- Has comparative SRH of men and women aged 25 to 34 changed over the period 1990 to 2014 and if so, in what way?
- Have physical activity in leisure time, educational level, Body Mass Index, depressive feelings, anxiety and satisfaction with economy changed in the age group during the same period?
- Do associations between comparative SRH and physical activity in leisure time, educational level, Body Mass Index, depressive feelings, anxiety and satisfaction with economy show the same pattern for men and women?
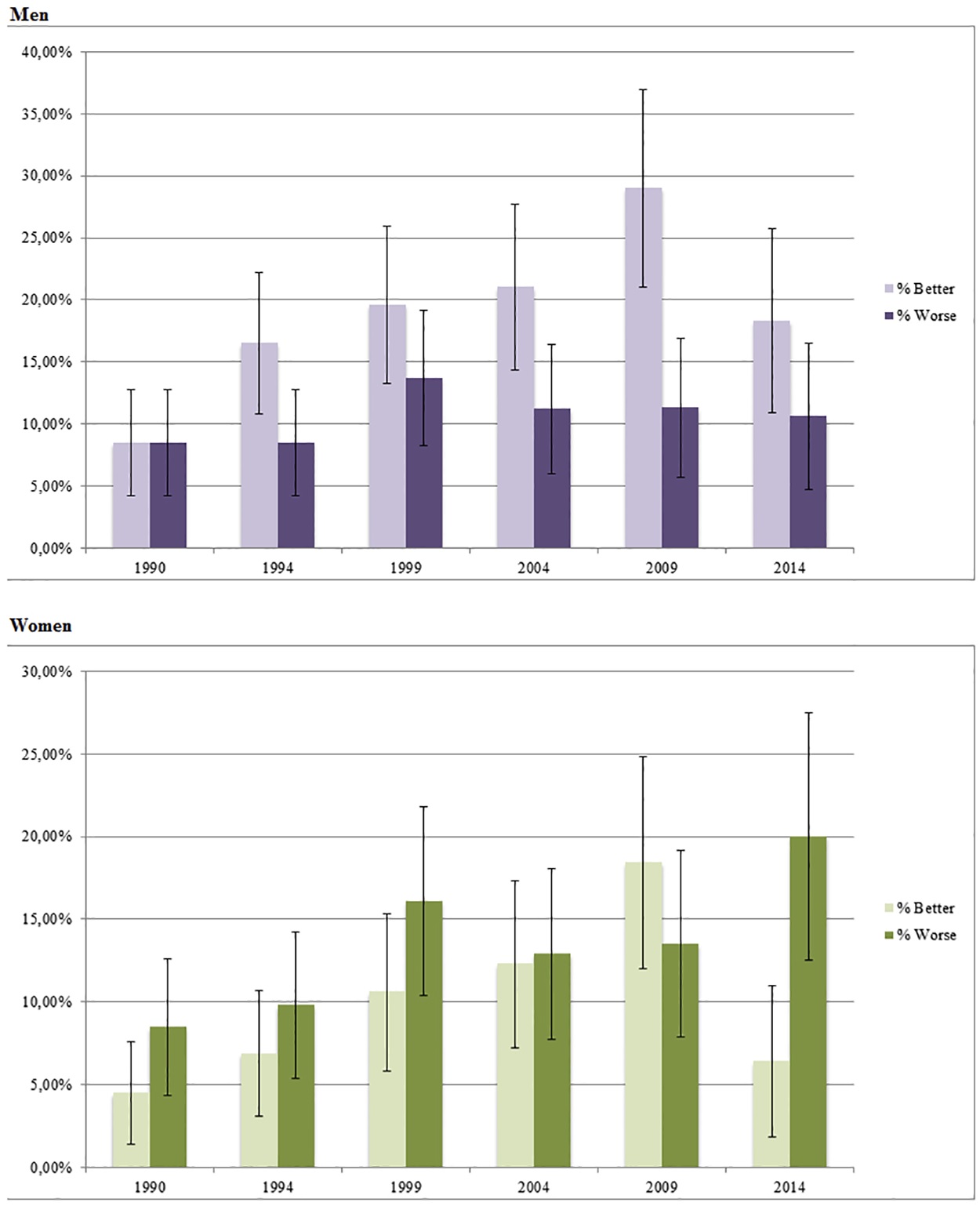
Conclusion
Time-trends of comparative self rated health 1990–2014 in the Northern Sweden MONICA Study show an increase of women rating their health as worse whereas men increased the proportion rating better. Physical activity in leisure time, educational level, BMI, depressive feelings, anxiety and dissatisfaction with economy have also increased during the period. Time trends for these variables show the same pattern for men and women. Our findings point to that gender aspects of SRH need to be further explored.